LASIK: 8 myths put to the test

Many myths circulate about LASIK, often inherited from the early days of refractive surgery or from second-hand accounts. They keep alive fears that are sometimes unfounded. In short: LASIK is a codified and extensively studied procedure, but it is neither magic nor free of precautions. Here are eight common claims, set against what the data and practice actually say.
Straight answer: fact versus fiction in one minute
Key point. No, LASIK does not cause blindness, and moving the eyes does not make the laser « miss », thanks to automatic eye tracking. Yes, the correction is lasting, even if slight change remains possible over time. Discomfort after the operation is generally brief. Dry eye is most often transient. The laser does not « burn » the eye, and a cataract remains operable later on. Like any surgery, LASIK involves precautions and contraindications: it is the role of the assessment to rule them out.
Refractive surgery · LASIK
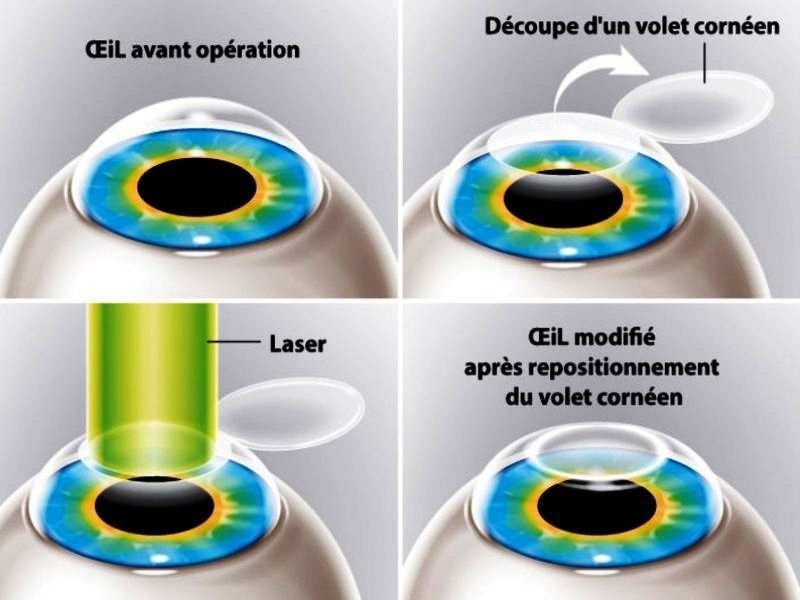
LASIK, step by step
Myth no. 1: « LASIK can cause blindness »
This is the most widespread fear, and the one furthest from reality. Blindness is not an expected complication of LASIK. The technique acts on the cornea, at the surface of the eye, and not on the retina or the optic nerve, which drive vision. Serious complications exist, as with any surgical procedure, but they are rare and most often manageable.
A ten-year follow-up covering myopia of up to -10 dioptres, for instance, reported no case of corneal ectasia, the most feared structural complication. The real answer to this fear is the pre-operative assessment, designed precisely to identify at-risk eyes and not to operate on them.
Myth no. 2: « If I move, the laser will miss »
Many imagine that a blink or a small movement of the eye could deflect the laser beam. In reality, current lasers are equipped with an eye-tracking system that analyses the position of the eye hundreds of times per second and adjusts the beam in real time.
If the eye moves out of the planned zone, the laser stops automatically and resumes as soon as it is recentred. Added to this are the local anaesthesia with eye drops and a small speculum that holds the eyelids: you cannot « close the eye » at the wrong moment. Involuntary movement is therefore managed by the machine, not left to chance.
Myth no. 3: « The effects do not last, the myopia comes back »
The correction obtained by LASIK is lasting. The reshaped cornea stays that way, and refraction stabilises within the first months. Over the long term, slight change is possible: in the ten-year follow-up already cited, around 73% of eyes stayed within one dioptre of the target and 92% within two dioptres, with a very small mean regression.
This change is more marked for high myopia. It is therefore not a « return of the myopia » as such, but a slow and limited drift, which may in some cases justify a touch-up. Moreover, LASIK does not prevent presbyopia from appearing with age: this is a distinct phenomenon, linked to the crystalline lens.
Myth no. 4: « It is a very painful operation »
The procedure is carried out under local anaesthesia with simple drops: during LASIK, what you feel is mainly a pressure and a passing drop in vision, rather than pain. It is in the hours that follow that discomfort most often arises, a gritty sensation, tingling, watering, sensitivity to light, which generally lasts 24 to 48 hours and eases with the prescribed eye drops.
PRK, a surface procedure, on the other hand causes slightly longer discomfort. To speak of torture would therefore be a great exaggeration; to speak of perfect comfort would be just as much. The reality lies between the two: transient discomfort, generally well tolerated.
Myth no. 5: « Dry eye is permanent »
Dry eye is the most frequent side effect of LASIK, but it is most often transient. It is explained by the temporary severing of small corneal nerves, which then gradually regenerate.
Very common in the first weeks, it diminishes over the months; dryness persisting beyond six months concerns a minority of patients, on the order of 20% according to studies, and mainly affects those who already had dry eyes before the operation. It is precisely for this reason that the ocular surface is evaluated and treated before operating. Our dedicated article details dry eye after LASIK.
Myth no. 6: « LASIK is only for mild myopia »
LASIK corrects a wide range of corrections: myopia, hyperopia and astigmatism. The ten-year follow-up already mentioned covered myopia of up to -10 dioptres. The limit is therefore not so much the figure of the correction as the anatomy of your eye: thickness and regularity of the cornea, above all. When the cornea is too thin or the myopia too high for a corneal laser, other solutions take over, such as the phakic implant (ICL) or SMILE. To say that LASIK is « only for mild myopia » is therefore inaccurate: it is the assessment that sets the limits, case by case.
Myth no. 7: « The laser burns the eye »
The image of the laser that « burns » is misleading. The excimer laser used to sculpt the cornea is a so-called « cold » laser: it does not heat the tissues but breaks the molecular bonds of the cornea with great precision, layer by layer, in a few tens of seconds. There is no flame, no burn, no smell of flesh. This photoablation is one of the principles that make refractive surgery so reproducible: each pulse removes a minute and controlled thickness of tissue.
Myth no. 8: « After LASIK, you can no longer operate on cataract »
This is false: having been operated on with the laser in no way prevents you, years later, from benefiting from cataract surgery. The only point to watch is technical: because LASIK altered the curvature of the cornea, calculating the power of the implant to be placed during the cataract operation is a little more delicate. But dedicated calculation formulas have been developed for these eyes and deliver good precision. Keeping the measurements of your eye taken before LASIK also helps this calculation. In short, LASIK closes no door for the future.
FAQ
Frequently asked questions
Is LASIK dangerous?
LASIK is a codified and extensively studied surgery. Like any surgical procedure, it involves risks, but serious complications are rare. Safety rests above all on the pre-operative assessment, which rules out at-risk eyes. Blindness is not an expected complication.
Can myopia come back after LASIK?
The correction is lasting. Slight change remains possible over many years, more marked for high myopia, and can sometimes justify a touch-up. It is not a true return of the myopia, but a slow and limited drift.
Does the operation hurt?
During the procedure, under anaesthesia with eye drops, what you feel is mainly pressure. Discomfort (a gritty sensation, watering) then arises and generally lasts 24 to 48 hours after LASIK, eased by the eye drops. PRK causes slightly longer discomfort.
Is dry eye after LASIK permanent?
Most often no. It is mainly transient and eases over the months, while the corneal nerves regenerate. Dryness persisting beyond six months concerns a minority of patients, especially those already prone to dryness before the operation.
Can high myopia be operated on with the laser?
Often yes: LASIK has been studied up to -10 dioptres. The limit depends mainly on the thickness and regularity of the cornea. When the corneal laser is not suitable, the phakic implant (ICL) or SMILE can take over, after evaluation.
Is moving the eye during the laser risky?
No. The laser has eye tracking that analyses the position of the eye hundreds of times per second and stops if the eye moves out of the planned zone, before resuming on recentring. A speculum also holds the eyelids open.
Does LASIK interfere with a future cataract operation?
No, cataract remains operable after LASIK. The only technical point is that calculating the implant is a little more complex, because the cornea has been reshaped. Dedicated formulas deliver good precision, and keeping your pre-LASIK measurements is helpful.
Scientific sources
- Alió JL, Muftuoglu O, Ortiz D, et al. Ten-year follow-up of laser in situ keratomileusis for myopia of up to -10 diopters. Am J Ophthalmol. 2008;145(1):46-54. PMID 18154754.
- Shoja MR, Besharati MR. Dry eye after LASIK for myopia: Incidence and risk factors. Eur J Ophthalmol. 2007;17(1):1-6. PMID 17294376.
- Moshirfar M, Shah TJ, Skanchy DF, Linn SH, Durrie DS. Meta-analysis of the FDA Reports on Patient-Reported Outcomes Using the Three Latest Platforms for LASIK. J Refract Surg. 2017;33(6):362-368. PMID 28586495.
- Wang L, Koch DD. Intraocular Lens Power Calculations in Eyes with Previous Corneal Refractive Surgery: Review and Expert Opinion. Ophthalmology. 2021;128(11):e121-e131. PMID 32615201.
Further reading
- LASIK: procedure and after-effects
- Dry eye after LASIK
- PRK: surface surgery
- The pre-operative assessment
Refractive assessment at the Cachan practice · Tel. 01 45 47 08 11
In summary
LASIK suffers from many myths, often out of proportion. It does not cause blindness, automatic eye tracking manages the movements of the eye, and the correction obtained is lasting, even if slight change remains possible over the years. Discomfort after the procedure is generally brief, dryness most often transient, and the « cold » laser does not burn the eye.
Finally, a cataract remains perfectly operable later on. True caution does not lie in the fears: it lies in a rigorous pre-operative assessment, which determines who can be operated on, by which technique, and who should not be. Laser refractive surgery is performed at the Clinique Laser Victor Hugo, after a complete assessment at the Cachan practice.
This article is intended for information and educational purposes. It does not replace a medical consultation. Results and risks vary from one patient to another; only an individual evaluation can establish an indication.
Written and reviewed by Dr Moïse Tourabaly, ophthalmic refractive surgeon — former chief resident (Quinze-Vingts National Eye Hospital).
Last updated: July 4, 2026